|
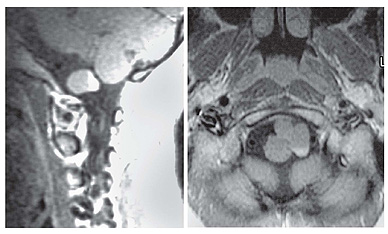
level was demonstrated inside the cyst in axial and sagittal T1 images: this finding has never been described as no enhancement usually occurs.(5,7) We suppose that a secretion of contrast inside the cyst has to be considered to explain this behaviour since epithelial columnar pattern indicating a foregut origin and secretory products have been found in pathology. DIFFERENTIAL DIAGNOSIS
Epidermoid cyst is a congenital disorder due an abnormal separation of the neural tube resulting in an epithelial inclusion cyst that has predominantly paramedian location, with density identical to CSF on CT; on MR, the signal relative to CSF is slightly hyperintense in T1 images, hyperintense in proton density, and iso-hyperintense in T2 (10), although high signal epidermoid cysts on T1-weighted MR images have been reported (11). Flair MR may be helpfull in differentiating epidermoid from arachnoid cyst, signals of epidermoid being similar to that of brain parenchyma, whereas that of arachnoids cyst are similar to spinal fluid(12). The low signal intensity of neurenteric cyst on diffusion-weighted images may enable differentiation from epidermoid cysts even if these cysts exhibit similar intensities on conventional MR images.(3) Dermoid cyst predominantly has a middline location and the density on CT and signal on MR are typically of fatty tissue. The correct preoperative diagnosis of NC may be difficult since the MR signals are variable, depending on the secretory products from the epithelial lining. In addition, the numerous synonyms for these cysts have caused a degree of confusion regarding their histogenesis. NC have histological features similar to cysts of neuroectodermal origin and thus need to be differentiated from choroidal and ependymal cyst. A practical subdivision is provided by Elmadbouth(9) into two main group: endodermal or neuroectodermal. Within the former category are epithelial cysts, which have a connective tissue stroma, are lined by cuboidal or columnar epithelium, but have no definite histologic evidence of origin. When they occur within the ventricular system they are termed colloid cysts; otherwise, they are called enterogenous or neurenteric or simply epithelial cysts. Ependymal and choroidal cysts fall into the second category. Light microscopy often fails to differentiate between these cysts: for example, cilia are common to both ependymal and enterogenous cysts and there is a histologic similarity between these two entities and colloid cysts. Electron microscopy helps to further differentiate. The walls of enterogenous cysts and colloid cysts are characterized by the presence of both columnar ciliated and nonciliated lining. The ciliated cells have no granular coating material. Nonciliated cells with microvilli are present in every case with characteristic surface granular glycocalyx coating. They possess features of secretory function, have prominent nuclei, and, in some cases, tight junctions are present. The appearance is similar to that of respiratory epithelium and is consistent with an endodermal origin. In contrast, cysts with ependymal and choroid plexus lining are composed of a single cell type and show no signs of keratinization, mucin production, or glycocalyx coating (9). Histochemical techniques suggest the origin of the cyst but do not provide a definitive diagnosis. | ||
| 5 | ||
 The
differential diagnosis of cystic masses in this region include arachnoid cyst,
epidermoid cyst, dermoid cyst; also the possibility of cystic neurinoma arising
from lower cranial nerves has to be considered. This latter possibility should
be distinguishable on the basis of contrast enhancement with ring-pattern due to
marginal solid rim tissue.
The
differential diagnosis of cystic masses in this region include arachnoid cyst,
epidermoid cyst, dermoid cyst; also the possibility of cystic neurinoma arising
from lower cranial nerves has to be considered. This latter possibility should
be distinguishable on the basis of contrast enhancement with ring-pattern due to
marginal solid rim tissue.