|
If the lesion is located in a cerebellar hemisphere and involves the dentate nucleus, the olivary
degeneration will be contralateral due to the decussation of the dentato-rubral
fibers. If the lesion is located in
the brainstem and involves the superior cerebellar peduncles at the level of
decussation, the degeneration
will occur bilaterally.
The microscopic changes underlying HOD are characterized by hypertrophy of degenerated
neurons followed by hypertrophy of astrocytes. The presence of proliferation of glial cells
(gliosis) is controversial.
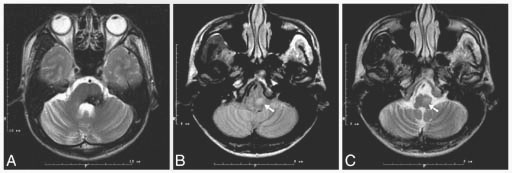
No change is seen on MRI images or on pathologic specimens within a week after the onset of ictus. A
hyperintense olive is demonstrable on PD/T2 weighted images 3 weeks after, corresponding to the pathological stage
of neuronal hypertrophy. Maximum hypertrophy of the olive is seen 5-15 months after the onset of ictus
and corresponds to an associated neuronal and glial hypertrophy.
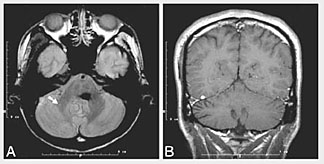
Because of projections from the inferior olivary nucleus to the contralateral cerebellum via the
inferior cerebellar peduncle (Fig1), contralateral cerebellar changes are associated with the
HOD. These changes
are characterized by atrophy and increased signal on PD/T2 weighted images of the dentate nucleus and
atrophy of the cerebellar cortex.
|