|
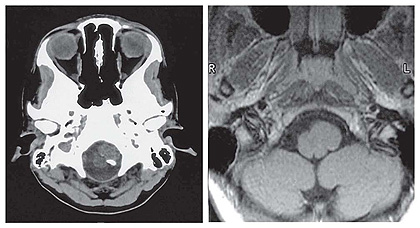
Neurenteric Cyst at the Cervico-Medullary Junction: Neuroradiological Findings, Histo-Pathological Correlations & Differential Diagnosis Drs Federica Denegri1, Marie-Christine Guiot & Denis Melançon 1Neuroradiologia, Ospedale CTO, Torino,Italy Neurenteric cyst (NC) are rare lesions occurring in the spinal canal, primarly in the cervico-thoracic spine; although they can occur anywhere from the cerebello-pontine angle to the coccyx, they are rarer in the posterior fossa or at the cervico-vertebral junction. We report a case of histologically proven neurenteric cyst an interesting MR finding of contrast fluid level inside the cystic lesion is probably explained by secretory function. CASE REPORT Neurological examination was normal. Blood tests obtained in the Emergency Room revealed no abnormality. The CT scan performed with and without contrast showed an oval mass, isodense to brain, at the level of the foramen magnum, with some coarse calcifications (Fig. 1A). There was no abnormality in the bone, nor contrast enhancement of the lesion. The MRI showed an intradural extra-medullary lesion, isointense in T1 (Fig. 1B), hyperintense in T2 and GR sequences (Fig. 2A, 2B), located in the anterior and left paramedian subarachnoid space, indenting slightly the medulla. A very thin tail arising from the cyst and going anteriorly was noted in all sequences. After gadolinium there was no real enhancement of the lesion but a iso-hyperintense fluid level pattern was seen inside the lesion in axial and sagittal T1 sequences.(Fig. 3A, 3B) The patient underwent a left posterior fossa craniotomy to remove the lesion thought to be most likely a dermoid cyst. The operative findings described a cystic lesion, ventral to the medulla, indenting it and displacing the 11th and 10th cranial nerves posteriorly. There was a very diaphanous cyst wall and the contents varied: some parts were semisolid and others contained a mucoid liquid. The cyst wall was adherent to cranial nerves and brainstem. There was no clear attachment to the dura. Once the cyst was collapsed and most of its wall removed, the cranial nerves and brainstem structures appeared unremarkable. The cyst measured approximately 1.5-2.0 cm in diameter.
| ||||
|
3 | ||||