|
Pilocytic Astrocytoma of
the Adult
Drs David M. Miller and Marie-Christine Guiot
Clinical History
 r. H.
is a 42 year old left handed male who suffered a witnessed generalized
seizure lasting 3-4 minutes. His past medical history was significant for
ethanol abuse as well as being followed at an outside institution for the
past three years for a seizure disorder. At the time of admission, his sole
prescription medication was dilantin. Physical exam was notable only for a
right parietal soft tissue hematoma. Neurological examination was normal.
Blood tests obtained in the Emergency Room revealed no abnormality. r. H.
is a 42 year old left handed male who suffered a witnessed generalized
seizure lasting 3-4 minutes. His past medical history was significant for
ethanol abuse as well as being followed at an outside institution for the
past three years for a seizure disorder. At the time of admission, his sole
prescription medication was dilantin. Physical exam was notable only for a
right parietal soft tissue hematoma. Neurological examination was normal.
Blood tests obtained in the Emergency Room revealed no abnormality.
Imaging Findings
|
|
Initial
non-enhanced CT scan of the brain (Fig. 1a,b) demonstrated a 4.2 x 3.8cm
left occipitoparietal cystic lesion without significant mass effect. Apart
from a right parietal soft-tissue hematoma there was no acute intracranial
traumatic injury identified. Following the injection of contrast (Fig 2a,b),
there is identification of a 1 cm. enhancing nodule at the medial aspect of
the lesion.
On MRI (Fig. 3), the left occipitoparietal lesion is again noted with a
homogeneous medial enhancing nodule again noted. There was no enhancement
identified along the wall of the cyst. Of further note is that the signal
intensity of the cystic component differs from that of clear fluid
representing proteinaceous material (Fig. 3b).
Discussion
In the pediatric
population, the pilocytic astrocytoma is both the most common cerebellar
neoplasm as well as the most common glioma overall- constituting 10% of all
pediatric astrocytomas(3). The quoted incidence rate within the
adult population varies across studies, with 0.49 per million per year the
incidence quoted in a recent British study specifically interested in adult
pilocytic astrocytomas (Bell, 2004).
One of the earliest features of
pilocytic astrocytomas in the adult to be recognized was how the
distribution of lesion location within the brain differed from the pediatric
population. In children, the cerebellum was the most frequent site of tumor
involvement (67%). In adults, however, Bell et al.(1) found that
five of the ten patients over
|
|
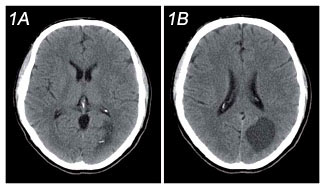
Figure 1: A,
Unenhanced
axial CT scan image at the level of the basalganglia demonstrates a left
occipital hypodense focus with a possible nodule at the medial aspect B,
Unenhanced image slightly cephalad to (a) shows a well defi ned left
parietoccipital cystic lesion that is slightly hyperdense to CSF.
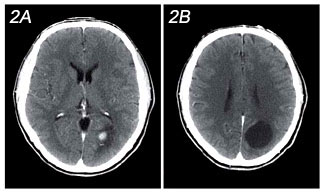
Figure 2: a,b
Contrast-enhanced CT matched images to Figure 1demonstrates homogeneous
enhancement of the medial mural nodule with no signifi cant enhancement of
the cystic component.
|
|
30 with pilocytic
astrocytomas had supratentorial lesions and the remaining five had
cerebellar lesions. Similarly, Burkhard et al(2) found
supratentorial involvement in 55% of adult patients. As would be expected
from the diverse location of the lesions, the clinical presentation is
varied depending on the site of the tumor.
The classic imaging manifestation of cerebellar and cerebral pilocytic
astrocytoma is that of a cyst-like mass with an enhancing mural nodule and
is seen in approximately two-thirds of cases. The cyst wall can |